
Co-contraction and empowerment with the Allyane method
Chloé is 20 years old. 5 years ago, she fractured her olecranon and was immobilized with an elbow to the body. Since then, she has struggled with limitations in extension and flexion (-20° in each amplitude). When Chloé extends her elbow, no matter how hard she tries, nothing works and she retains her deficit. Yet on X-ray, there's nothing to explain this bone problem.
The reason for this restriction is in fact an almost simultaneous co-contraction of the extensors and flexors of the elbow with a predominance of the muscle...biceps in extension and triceps in flexion. As this contraction is greater than that of the triceps during extension, Chloe cannot fully extend her elbow. Similarly, when she tries to bend her elbow, the triceps contraction at the end of the movement is greater than that of the elbow flexors.

Definition
" Muscle co-activation or co-contraction is a phenomenon describing the simultaneous activation of two agonist/antagonist muscles during a movement. Muscle co-activation is useful for limiting the range of motion and increasing precision"(1)
Advantages and disadvantages of co-contraction
In some cases, this co-contraction is necessary to protect the joint in a range that is momentarily deleterious to use. In Chloe's case, the last twenty degrees of flexion or extension were likely to cause pain during the remission phase of her fracture.
The problem is that this safe range of motion has been maintained and this has set up a blurring of the full flexion and extension pattern of the elbow, with the muscles acting protectively as if the joint was coming to a maximum in both directions.
As a result, at the end of extension, the flexors contract, leading not only to a blocking of the joint but also to a decrease in the strength of the extensors (as if the agonist/antagonist action was reversed).
What is done in rehabilitation
Muscle structures
"Flexor-extensor and pronator-supinator co-contractions frequently occur in the early stages, limiting mobility. Active contract-release techniques are used while respecting the painful arc.
Biofeedback allows the patient to visualise co-contractions during movements and to become aware of muscle relaxation.
Protective reflex contractures can also increase amplitude limitations and isometric or excitomotor muscle contraction (1 Hz with intensity causing muscle twitching) can break the vicious pain/contraction cycle and gain a few degrees. (2)
These rehabilitation techniques work in most cases, but for Chloe it was not successful because the motor pattern for her elbow movement remained disrupted.
What neuromotor reprogramming offers
Allyane is an innovative method based on low-frequency sounds, proprioceptive sensation and mental imagery.
In this way, we do not start from the gesture to change it but from the image of what a corrected gesture would be.
"The motor disorder is not of deficit origin but comes from a dysfunction of the motor realization".
Julian de AJURIAGUERRA
You are a practitioner and would like more information on the Allyane method and our training courses?
Awareness of the gesture to be modified
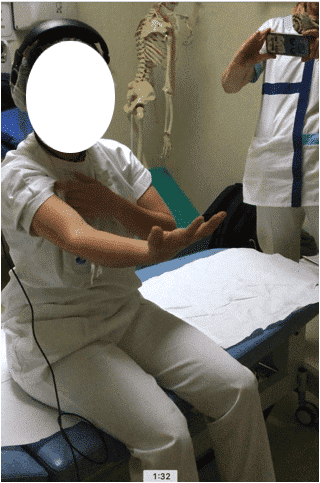
In order to ensure that the negative image of the existing movement is perceived as such, we will first materialise it by asking the patient to perform the movement to be modified, possibly comparing it with the healthy side if necessary. The patient will be helped to identify all the proprioceptive sensations associated with this movement.
When he performs the latter he feels, and therefore constructs, proprioceptive information about the gesture to be changed.
Then, to create the motor image, the patient imagines doing the gesture with the sensations he has just created.
Listening to low frequency sounds
Once the motor imagery construction of proprioceptive sensations of the gesture to be changed has been established, the patient listens to sequences of low-frequency sounds using headphones and the Alphabox®, which generates Pulsed Sound (PS).
These specific sounds will increase the emission of alpha brain waves and modulate brain activity, notably by hyper-activating its motor areas.
This phase takes about 5 minutes.
Construction of the motor image of the healthy gesture
For Chloe, it will be a question of becoming aware on the healthy upper limb that when she performs an extension of the elbow slightly resisted by the therapist, only her triceps comes into action and her biceps is completely relaxed.
As with the construction of the negative image, once the sensations of good biceps relaxation and good triceps contraction are felt by the patient, we ask them to create this good motor image.
Chloe therefore imagines performing this movement by feeling all the proprioceptive information she has just accumulated.
Clearance phase
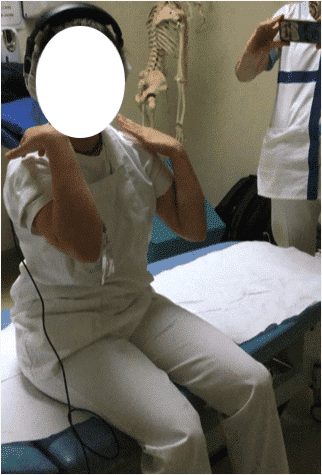
At this stage, we ask the patient to recall the negative sensation she had built up at the beginning of the session with this progressive increase in the involuntary contraction of the biceps when extending the elbow (mental image of the gesture to be changed)
Once this reminder has been made and felt, Chloe is guided by the therapist and mentally erases not only this sensation but also the whole of the "pathological" upper limb to which a specific frequency sound is associated.
This is the phase of deprogramming (or deleting) the gesture to be modified.
Reprogramming phase
Once the erasure is complete, we ask the patient to "reconstruct" her new arm with the good proprioceptive sensations of the healthy arm previously stored.
That is, it produces the motor image of proprioceptive sensations of an elbow that can go to extension and is capable of full amplitude since the biceps is completely relaxed at the end of the movement.
When she confirms this good motor image of the movement, we validate this information by listening to an Associated Sound.
This reprogramming phase is repeated three times before the actual movement is performed.
In the case of this young girl, we can see that the recovery is total for the elbow extension.
We therefore go back to work to recover the flexion which, through the same process of co-contraction at the end of the amplitude, remains deficient.
End of session analysis
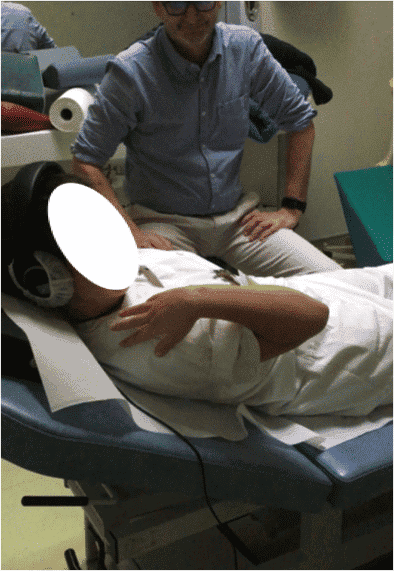
Once the three repetitions of the previous phase have been completed, we ask Chloe to actually do the movement;
At this stage we analyse the progress made since the beginning of the session

End of session anchoring
Once flexion and extension have been recovered, the treatment continues with an anchoring phase. During this phase, pulsed sounds (SP) and associated sounds (SA) are played in the headphones in succession so that the work done is memorised at the cerebral level.
This phase takes about ten minutes.
What next?
It is important for Chloe to work on this arm movement to get into these new amplitudes, even if exploring these new angulations is initially uncomfortable.
Indeed, it is necessary to preserve this new engine scheme so that it can endure!
Are you a movement professional (doctor, physiotherapist, osteopath,...) and would like to know more about the detection of motor inhibitions? Visit our professional page.
You can also contact us at 04 28 29 58 10 or contact@allyane.com.
Source:
Rehabilitation of radial head fractures: stability-mobility compromise Yannick Dauce*, Béatrice Chapin-Bouscarat* Kiné Scientifique n°415 octobre 2001